*touchwood*
If one day you are smothered by someone n you are still conscious at that moment, u should struggle violently? or you shouldn't do that?
There will be 2 outcomes of struggling:
a) There will be abrasions on the face/nose or contusions of the lips due to the pressure of the palm. Therefore, when your dead body is examined by forensic doctors, he/she can suspect that your death is due to homicidal smothering.
b) You will die faster due to increased utilization of oxygen.
BUT,
if you don't struggle, you will leave no evidence to the forensic doctor. The autopsy will fail to disclose any injuries. He/she cannot find evidence to prove that you are dead due to homicidal smothering.
Conclusion,
If this happen to you, it is better for you to struggle violently :p oh yea, make sure u build up emotion intensively, so there may be cadaveric spasm after u die.
Reference:
1) Dimaio V.J and Dimaio D, 2001. Forensic Pathology 2nd edition. Boca Raton, London. CRC Press.
Thursday, December 30, 2010
Thursday, December 9, 2010
I want to tell u story
Hardly remember the name of the drugs against Influenza A?
Let me tell you story about adamantanes and neuraminidase inhibitors.
Once upon a time, there were 2 families: adamantanes and neuraminidase inhibitors. Adamantanes have 2 children: aman (amantadine) and raman (ramantadine).
One day neuraminidase inhibitors met adamantanes and his 2 children in Pogung Baru.
 "Hello Adam. Are they your children? They are very cute!" said neuraminidase inhibitors.
"Hello Adam. Are they your children? They are very cute!" said neuraminidase inhibitors.
"Yes, they are. I heard that you have married few years ago. So, do you have any children?" asked adamantanes.
"Yea, I have two also. One is named Zana (zanamivir) and another is named as oselta (oseltamivir)," said neuraminidase inhibitors with his lips curved into a smile.
"So, how is your life now? Do you....still contact with Influenza A?" asked adamantanes.
"Yeah, I'm working with him now. He is my boss. As always, he is still as irritating as last time in the class. Do you still remember how he bullied us last time?" said neuraminidase inhibitors.
 "Of course I remember! And recently, he had annoyed me very much. He made my ducks and pigs sick by injecting them with virus! I wanna revenge! However, I hardly approach him as he has already known that I wana take him down (drug-resistant). I need someone to help me. Since you hate him so much and he doesn't know this ( less likely to promote drug resistance), you still stand a chance to approach him and to defeat him. How about we have a conspiracy?" said adamantanes.
"Of course I remember! And recently, he had annoyed me very much. He made my ducks and pigs sick by injecting them with virus! I wanna revenge! However, I hardly approach him as he has already known that I wana take him down (drug-resistant). I need someone to help me. Since you hate him so much and he doesn't know this ( less likely to promote drug resistance), you still stand a chance to approach him and to defeat him. How about we have a conspiracy?" said adamantanes.
"Why not? Count me in, dude! We should work this out together!" said neuraminidase inhibitors.

Hopefully this story helps you. This is the way I memorize the drugs and which one will create drug resistant.
Hope you enjoy reading this story.
Reference:
1) Dr. Titik Nuryastuti. Lecture: New Emerging Disease Avian Influenza Coronavirus/SARS.
Let me tell you story about adamantanes and neuraminidase inhibitors.
Once upon a time, there were 2 families: adamantanes and neuraminidase inhibitors. Adamantanes have 2 children: aman (amantadine) and raman (ramantadine).
 |
| Assume they are amantadine and ramantadine :p |
"Yes, they are. I heard that you have married few years ago. So, do you have any children?" asked adamantanes.
"Yea, I have two also. One is named Zana (zanamivir) and another is named as oselta (oseltamivir)," said neuraminidase inhibitors with his lips curved into a smile.
"So, how is your life now? Do you....still contact with Influenza A?" asked adamantanes.
"Yeah, I'm working with him now. He is my boss. As always, he is still as irritating as last time in the class. Do you still remember how he bullied us last time?" said neuraminidase inhibitors.
"Why not? Count me in, dude! We should work this out together!" said neuraminidase inhibitors.
------- The end----------
Hope you enjoy reading this story.
Reference:
1) Dr. Titik Nuryastuti. Lecture: New Emerging Disease Avian Influenza Coronavirus/SARS.
Wednesday, December 8, 2010
Nosocomial infection: whose fault?
A 60-year-old lady was admitted with the complain of epigastric pain and dyspnea. She was previously admitted for few times with the same complain. The ECG was normal and other examinations were within normal limit. The doc suspected she had peptic ulcer. On the 3rd day of admission, she had fever and back pain. On examination, renal punch on left side was positive. The urinalysis showed that leukocytes +, granulocytes level increased. She was then treated as UTI.
At first, the patient had epigastric pain and dyspnea. The patient was then hospitalised due to the unrelieved pain and dyspnea. On the third day, she suddenly had UTI. Why did the patient suddenly had UTI? What do you think? Nosocomial infection? Do you agree?
There are two types of nosocomial infection:
a) endogenous infection: the causative agents comes from the patient and the infection develop during hospitalization as a result of the patient's decrease of resistance.
b) cross contamination followed by cross infection: the patient comes into contact with new infective agents and develops infection.
Source of nosocomial infection:
a) Human: patients, hospital workers
b) Environment: water, air, waste, food, device (endoscope, ventilator), dust
a) The microbial agent
b) Patient suscepbility
c) Environmental factors
d) Bacterial resistance
If you look at the source and the factors, you will find that we can actually blame a lot of parties:
a) Blame the patient! why do they become weak? Comon, make ur immune system stronger!
The patient may say: "errr...why do you blame me? I can't help with this! I've already kept the environment clean and always eat healthy food. But, still, I am infected! And maybe you have to blame the doctors! They are the cause!"
b) Blame the hospital workers:
c) Blame the microorganisms! why do they need to develop a resistant strain? why do they invade the human body?

I don't think doctors should be blamed. The main point is DOCTOR is NOT THE ONLY PARTY responsible for this, but ALL PARTIES. How sure are you that the doctor is the factor or the only factor for causing nosocomial infection? How if it is not the doctors' fault, but the nurse or the patient themselves for being too weak? How if the infection is transmitted through dust, air, food, water, but not from the human? So, forget about it. Stop blaming each other. It s better that we human take actions in preventing this-Do it hand in hand!
1) Do a surveillance. Perform antibiotic susceptibility test and monitor the trends in prevalence of bacterial resistance to antimicrobial agent.
2) Based on the surveillance, make a list of antiobiotics in which the doctor can prescribe to the patients.
3) Doctors should prescribe narrow spectrum of antibiotics if possible; When waiting for lab test result, apply empirical treatment/ based on guidelines.
4) Use prophylactic antibiotic only in situation where proved valuable.
5) Sterilization
6) Disinfection, eg fogging.
7) Avoid environmental contamination: Maintain the environmental hygiene and sanitation.
8) Use containment isolation procedures for patient infected with resistant organism.
9) Aseptic hand washing procedures.
10) Safe injection method.
11) Apply crop rotation policy: It is used for predetermined period (e.g. 3 months) and rotated to another antibiotic after 3 Mo and another after 3 Mo and finally recycled.
12) Ensure personal hygiene.
13) Wear gloves, mask, etc.

Let's do these together ;)
Reference:
1) Prof. Dr. Irwan Dwiprahasto. Lecture: Pharmocology: Drugs Formulary and Antibiotic Hospital Policy.
2) Dr. Hera Nirwati. Lecture: Nosocomial Infections.
At first, the patient had epigastric pain and dyspnea. The patient was then hospitalised due to the unrelieved pain and dyspnea. On the third day, she suddenly had UTI. Why did the patient suddenly had UTI? What do you think? Nosocomial infection? Do you agree?
There are two types of nosocomial infection:
a) endogenous infection: the causative agents comes from the patient and the infection develop during hospitalization as a result of the patient's decrease of resistance.
b) cross contamination followed by cross infection: the patient comes into contact with new infective agents and develops infection.
Source of nosocomial infection:
a) Human: patients, hospital workers
b) Environment: water, air, waste, food, device (endoscope, ventilator), dust
Factors that contribute to this development of nosocomial infection:
a) The microbial agent
b) Patient suscepbility
c) Environmental factors
d) Bacterial resistance
SO, for nosocomial infection cases, whose fault? Can the patients sue the doctors?
If you look at the source and the factors, you will find that we can actually blame a lot of parties:
a) Blame the patient! why do they become weak? Comon, make ur immune system stronger!
The patient may say: "errr...why do you blame me? I can't help with this! I've already kept the environment clean and always eat healthy food. But, still, I am infected! And maybe you have to blame the doctors! They are the cause!"
b) Blame the hospital workers:
- Doctors: Blame them for giving antibiotcs to the patients. Blame them for using devices,like endoscope, when examing the patients. Blame them for asking the nurses giving them IV line, giving injection.....
- Nurses: Blame them for not using antiseptic procedures! Blame them for not washing hands!
- Hospital cleaners: Blame them for not mopping the floor every hour! Blame them for not empty the bin every hour!
c) Blame the microorganisms! why do they need to develop a resistant strain? why do they invade the human body?
Therefore,
I don't think doctors should be blamed. The main point is DOCTOR is NOT THE ONLY PARTY responsible for this, but ALL PARTIES. How sure are you that the doctor is the factor or the only factor for causing nosocomial infection? How if it is not the doctors' fault, but the nurse or the patient themselves for being too weak? How if the infection is transmitted through dust, air, food, water, but not from the human? So, forget about it. Stop blaming each other. It s better that we human take actions in preventing this-Do it hand in hand!
What are the prevention?
1) Do a surveillance. Perform antibiotic susceptibility test and monitor the trends in prevalence of bacterial resistance to antimicrobial agent.
2) Based on the surveillance, make a list of antiobiotics in which the doctor can prescribe to the patients.
3) Doctors should prescribe narrow spectrum of antibiotics if possible; When waiting for lab test result, apply empirical treatment/ based on guidelines.
4) Use prophylactic antibiotic only in situation where proved valuable.
5) Sterilization
6) Disinfection, eg fogging.
7) Avoid environmental contamination: Maintain the environmental hygiene and sanitation.
8) Use containment isolation procedures for patient infected with resistant organism.
9) Aseptic hand washing procedures.
10) Safe injection method.
11) Apply crop rotation policy: It is used for predetermined period (e.g. 3 months) and rotated to another antibiotic after 3 Mo and another after 3 Mo and finally recycled.
12) Ensure personal hygiene.
13) Wear gloves, mask, etc.
Let's do these together ;)
Reference:
1) Prof. Dr. Irwan Dwiprahasto. Lecture: Pharmocology: Drugs Formulary and Antibiotic Hospital Policy.
2) Dr. Hera Nirwati. Lecture: Nosocomial Infections.
Sunday, December 5, 2010
Should Dr.Sardjito General Hospital be fined or given a warning letter?
Yesterday, when I was walking into IRNA I of Dr. Sardjito Genaral Hospital, I saw a lot of people (more than 10 ppl) smoking outside IRNA I.

Wow, more than 10 people smoked in the hospital compound!!
For your information, one of the obligations of a hospital is to enforce all hospital environment as non-smoking area. Administrative sanction will be imposed upon those hospitals which refuse to fulfil the obligation. The sanction can be:
Reference:
1. MOH. Guest lecture: Hospital Law (Legal Aspect of Hospital)
Wow, more than 10 people smoked in the hospital compound!!
For your information, one of the obligations of a hospital is to enforce all hospital environment as non-smoking area. Administrative sanction will be imposed upon those hospitals which refuse to fulfil the obligation. The sanction can be:
- warning
- written warning
- fine and cancellation of hospital permit
Reference:
1. MOH. Guest lecture: Hospital Law (Legal Aspect of Hospital)
Friday, December 3, 2010
I'll help you to tell your family who you are
"I'm Dr.O. i'll strain all my nerves to find out your identity...I'll help you to tell your family who you are!"
Whose identity???
A burnt dead human.
wow, this is the job of a forensic anthropologist. They are gotta identify the dead when the victims are with unrecognizable face and bone exposure or the body is mutilated or only part of the body is found.
Scenario:
No. 46-102/40 was unrecognised because the victim was burnt. So, Dr. O, a forensic anthropologist, was asked to identify the victim.
So, what does "46-102/40" means?
It means body number 46 removed from the site at grid co-ordinate 102/83.
If it is "46P-102/40", what does it mean? How about "M46"?
"46P-102/40" means body part number 46 removed from the site at grid co-ordinate 102/40; "M46" means body or part number 46 which was labelled at the mortuary and therefore no co-ordination was written down when labelling.

The forensic anthropologist is gonna identify the race, stature, sex, and age of the victim.
1) Race.
The picture below is the skull of 46-102/40. So can you identify the race of the victim? (I have circled the important characteristic, hope this can lead you to have some idea)


"The skull is keeled and brachicephalic (short but broad skull). The major suture of the skull is complex.The orbits are round and the nasal is slightly depressed. The nasal spine is moderate. The victim has projecting zgmomatics and malar tubercle. Besides that, the zygomaticomaxillary suture is angled. The dentition is edge-to-edge bite and the buccal pits are obeseved. The victim's face has everted gonion angle.Therefore, the victim is identified as mongoloid."
What about the other characteristic of mongoloid? Let's look at the picture below.

How do you know that is not caucasoid or negroid? Let's look at the picture below.
So the picture above is caucasoid. The important features are:
 "The humerus length is 31 cm. So, the stature is estimated between 160.16 and 168.66cm"
"The humerus length is 31 cm. So, the stature is estimated between 160.16 and 168.66cm"
To estimate the stature, we usually use humerus. But if humerus is not found, other long bones will be used, such as femur. Caliper is used to measure the length of long bone. There are different formula for different long bone. We then substitute the length of the long bone into the formula. After that, calculate it to get the range.
3) Sex
"The pelvic inlet is small and looks like a heart shape. The subpubic angle is acute (70 degree). The ventral anterior margin of the obturator foramen is sharp. The acetabulum is wide and deep, facing laterally. Besides that, the sciatic notch is angled ,deep and narrow. The ilium is vertical (stand up). The fossa auricularis is long, and narrow, curving anteriorly.There is no parturition pits, nor the preauricular sulcus. By examining the skull, I find that the supraorbital ridge is prominent and is not smooth. The mastoid process is large. So, the victim is identified as a male."
The picture below shows how a female pelvic looks like.
Further reading: Tortora G.J., Derrickson B. Principles of Anatomy and Physiology. John Wiley & Sons, Inc. 11th edition, 2006. Page 244.
We can also identify sex through secondary sexual signs, e.g. mammae; cranial bone; and sex chromosome.
4) Age.

"By using the dental attrition, the estimated age of the victim is 30-35 years old"
For the burnt dead victims, teeth is important in identification. For the dental atrition, the concept is as one grows older, there will be more enamel loss.
However, there is factor which influencing the accuracy of using this method. Humans eat a variety of food which promote enamel attrition at different rates. Therefore, this may influence the result of estimating the age.
Besides using dental attrition, dental formation and eruption times is used in estimating age to approximately 15 years. For the old age, can try to identify the changes of bone due to arthritis or osteoporosis and their orbits are lipping.
To estimate age, we can also use pubic symphysis.

Another alternative is we access the bone growth.
So, 46-102/40 is identified as a mongoloid male, whose stature is between 160 and 169cm, with estimated age 30-35 years old. To find his identity, we need the ante-mortem data and further lab test, e.g. DNA, and then we will do the reconciliation.
Reference:
1) Prof. drg. Etty Indriati. Lecture: The Roles of Anthropology in Disaster Victim Identification.
2) Dr. Yudha Nurhantari. Lecture: Management of Dead Victims in Mass Disaster.
3) http://people.wku.edu/darlene.applegate/forensic/lab9/lab9.html (Identify race)
4) http://www.the-crankshaft.info/2010/07/morphological-age-estimation.html
5) http://www.interpol.int/public/DisasterVictim/guide/chapitre4.asp
6) http://medical-dictionary.thefreedictionary.com/dolicocephalic+skull
7) http://education.yahoo.com/reference/gray/subjects/subject/58 (Female pelvis)
8) http://en.wikipedia.org/wiki/Pelvis
9) http://www.wadsworth.com/anthropology_d/special_features/forensics/forensics_index/index.html (Role of forensic anthropologist)
10) Tortora G.J., Derrickson B. Principles of Anatomy and Physiology. John Wiley & Sons, Inc. 11th edition, 2006. Page 244.
11) Practical Guide Block 4.2: Forensic Anthropological Identification of Disaster Victims.
Whose identity???
A burnt dead human.
wow, this is the job of a forensic anthropologist. They are gotta identify the dead when the victims are with unrecognizable face and bone exposure or the body is mutilated or only part of the body is found.
Scenario:
No. 46-102/40 was unrecognised because the victim was burnt. So, Dr. O, a forensic anthropologist, was asked to identify the victim.
So, what does "46-102/40" means?
It means body number 46 removed from the site at grid co-ordinate 102/83.
If it is "46P-102/40", what does it mean? How about "M46"?
"46P-102/40" means body part number 46 removed from the site at grid co-ordinate 102/40; "M46" means body or part number 46 which was labelled at the mortuary and therefore no co-ordination was written down when labelling.

The forensic anthropologist is gonna identify the race, stature, sex, and age of the victim.
1) Race.
The picture below is the skull of 46-102/40. So can you identify the race of the victim? (I have circled the important characteristic, hope this can lead you to have some idea)

"The skull is keeled and brachicephalic (short but broad skull). The major suture of the skull is complex.The orbits are round and the nasal is slightly depressed. The nasal spine is moderate. The victim has projecting zgmomatics and malar tubercle. Besides that, the zygomaticomaxillary suture is angled. The dentition is edge-to-edge bite and the buccal pits are obeseved. The victim's face has everted gonion angle.Therefore, the victim is identified as mongoloid."
What about the other characteristic of mongoloid? Let's look at the picture below.

How do you know that is not caucasoid or negroid? Let's look at the picture below.
 |
| Caucasoid skull |
- dolicocephalic skull (long but narrow skull)
- the major suture is simple
- sloping orbits
- narrow nasal aperture; tower nasal; deep nasal sill and large nasal spine
- s-shaped zygomaticomaxillary suture
- retreating zygomotics
- the face has straight gonion angle
The picture above is negroid skull. The important features are:
Negroid skull - the skull with post-bregmatic depression
- the major suture is simple
- s-shaped zygomaticomaxillary suture
- rectangular orbits
- guttered lower nasal border; wide nasal aperture; no nasal spine
- large prognathism

To estimate the stature, we usually use humerus. But if humerus is not found, other long bones will be used, such as femur. Caliper is used to measure the length of long bone. There are different formula for different long bone. We then substitute the length of the long bone into the formula. After that, calculate it to get the range.
3) Sex
 |
| Male pelvis |
The picture below shows how a female pelvic looks like.
 |
| female pelvis |
We can also identify sex through secondary sexual signs, e.g. mammae; cranial bone; and sex chromosome.
4) Age.
"By using the dental attrition, the estimated age of the victim is 30-35 years old"
For the burnt dead victims, teeth is important in identification. For the dental atrition, the concept is as one grows older, there will be more enamel loss.
 |
| Age estimation by using dental atrition |
Besides using dental attrition, dental formation and eruption times is used in estimating age to approximately 15 years. For the old age, can try to identify the changes of bone due to arthritis or osteoporosis and their orbits are lipping.
To estimate age, we can also use pubic symphysis.

Another alternative is we access the bone growth.
So, 46-102/40 is identified as a mongoloid male, whose stature is between 160 and 169cm, with estimated age 30-35 years old. To find his identity, we need the ante-mortem data and further lab test, e.g. DNA, and then we will do the reconciliation.
Reference:
1) Prof. drg. Etty Indriati. Lecture: The Roles of Anthropology in Disaster Victim Identification.
2) Dr. Yudha Nurhantari. Lecture: Management of Dead Victims in Mass Disaster.
3) http://people.wku.edu/darlene.applegate/forensic/lab9/lab9.html (Identify race)
4) http://www.the-crankshaft.info/2010/07/morphological-age-estimation.html
5) http://www.interpol.int/public/DisasterVictim/guide/chapitre4.asp
6) http://medical-dictionary.thefreedictionary.com/dolicocephalic+skull
7) http://education.yahoo.com/reference/gray/subjects/subject/58 (Female pelvis)
8) http://en.wikipedia.org/wiki/Pelvis
9) http://www.wadsworth.com/anthropology_d/special_features/forensics/forensics_index/index.html (Role of forensic anthropologist)
10) Tortora G.J., Derrickson B. Principles of Anatomy and Physiology. John Wiley & Sons, Inc. 11th edition, 2006. Page 244.
11) Practical Guide Block 4.2: Forensic Anthropological Identification of Disaster Victims.
Thursday, December 2, 2010
The dead
"A volcano eruption has just happened. A lot of people are dead. We need your help!"
When death is involved in a disaster, we need to identify the dead victims. Why? it is a respect of death person, and it is for the purpose of legal claims and obligation in relation to property, estate and debts.
So, who are in the disaster victim identification (DVI) team?
1) the police or interpol (international police)
2) forensic pathologist, anthropologist and dentist
3) army
4) trained volunteers
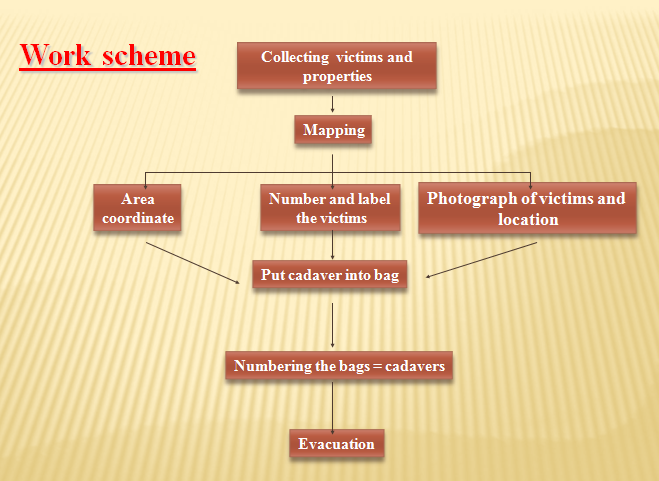
There are few procedures in DVI:
1) Phase I: Scene. The team will search for bodies, body parts, properties, mapping the area of disaster, labelling, documentation, putting the dead bodies in body bags.
 2) Phase II: Mortuary: Post-morten examination. They will do:
2) Phase II: Mortuary: Post-morten examination. They will do:
a) Documentation: bodies, body parts, properties.
b) External-internal examination, autopsy: forensic pathologist's job.
c) Identification of race, sex, age, stature: Forensic antropologist's job.
d) Dental examination: Forensic dentist and anthropologist's job.
e) Record body fragmentations: What body parts are missing.
f) Taking samples for DNA examination: blood, tissue, bone, teeth.
g) Taking roentgen of the upper and lower jaw with teeth.
All post-mortem examination data is recorded in pink form.
3) Phase III: Antemortem data compilation. The data is gathered from family members, friends, doctor, dentist (medical record for matching with the primary identification traits). The data can be vital signs, specific characters, jewelery, watch, clothes (for matching with secondary identification traits). All the antemortem data is recorded in yellow form.
4) Phase IV: Reconciliation. It is to compare antemortem data with postmortem data. Identification is confirmed when there is one primary identification method is matched (DNA, fingerprints, dental profile) or at least 2 secondary identification method are matched ( visual, photography, properties, medic-anthropology).When all parties provide evidence and proofs that matched/identified-->signed and dated.
5) Phase V: Release and debrief.

How if the dead body is unidentified?
According to Dr. Yudha Nurhantari, a victim is defined as "unidentified" when it is more than 48 hrs in the morgue. Usually during the period, the information or the photographs of the dead body is released to the media. According to Prof. Drg. Etty Indriati, in a disaster settings, if the dead body is unidentified after 3 days, mass burial will be done. They will be buried 2m in depth.

In DVI,
they say: The success indicator is not the the speed, but the accuracy
Reference:
1) Dr, Yudha Nurhantari. Lecture: Management of Dead Victims In Mass Disaster.
2) Prof. Drg. Etty Indriati. Lecture: The Roles of Anthropology in Disaster Victim Identification.
When death is involved in a disaster, we need to identify the dead victims. Why? it is a respect of death person, and it is for the purpose of legal claims and obligation in relation to property, estate and debts.
So, who are in the disaster victim identification (DVI) team?
1) the police or interpol (international police)
2) forensic pathologist, anthropologist and dentist
3) army
4) trained volunteers
There are few procedures in DVI:
1) Phase I: Scene. The team will search for bodies, body parts, properties, mapping the area of disaster, labelling, documentation, putting the dead bodies in body bags.
a) Documentation: bodies, body parts, properties.
b) External-internal examination, autopsy: forensic pathologist's job.
c) Identification of race, sex, age, stature: Forensic antropologist's job.
d) Dental examination: Forensic dentist and anthropologist's job.
e) Record body fragmentations: What body parts are missing.
f) Taking samples for DNA examination: blood, tissue, bone, teeth.
g) Taking roentgen of the upper and lower jaw with teeth.
All post-mortem examination data is recorded in pink form.
3) Phase III: Antemortem data compilation. The data is gathered from family members, friends, doctor, dentist (medical record for matching with the primary identification traits). The data can be vital signs, specific characters, jewelery, watch, clothes (for matching with secondary identification traits). All the antemortem data is recorded in yellow form.
4) Phase IV: Reconciliation. It is to compare antemortem data with postmortem data. Identification is confirmed when there is one primary identification method is matched (DNA, fingerprints, dental profile) or at least 2 secondary identification method are matched ( visual, photography, properties, medic-anthropology).When all parties provide evidence and proofs that matched/identified-->signed and dated.
5) Phase V: Release and debrief.
- Release. The dead body is released to the family member, along with the letter.
- Debrief: Compile documents. DVI team is dismissed.

How if the dead body is unidentified?
According to Dr. Yudha Nurhantari, a victim is defined as "unidentified" when it is more than 48 hrs in the morgue. Usually during the period, the information or the photographs of the dead body is released to the media. According to Prof. Drg. Etty Indriati, in a disaster settings, if the dead body is unidentified after 3 days, mass burial will be done. They will be buried 2m in depth.

In DVI,
they say: The success indicator is not the the speed, but the accuracy
Reference:
1) Dr, Yudha Nurhantari. Lecture: Management of Dead Victims In Mass Disaster.
2) Prof. Drg. Etty Indriati. Lecture: The Roles of Anthropology in Disaster Victim Identification.
Wednesday, December 1, 2010
What is disaster?
What is DISASTER?


Disaster is defined as sudden ecological phenomenon of sufficient magnitude to require external aids. It is also defined as an event or a series of events that are caused by natural factor or man-made factor, resulting in loss of human lives, environmental damage, loss of properties, and psychological problem. Consequently, human lives are harmed and disturbed.
Let's look at the conceptual framework of a disaster:

1) Hazard: Hazard is the cause of an event or a disaster. For example: the hazard of flood is the rain; the hazard of volcanic eruption is the volcano.
2) Risk: A factor which increases the probability of a hazard to become an event. For example: Deforestation will increase the probability of a flood to take place;
3) Event: It is caused by the hazard. For example: flood, volcano eruption.
4) Impact: When the event involves a population, but not yet a disaster. For example: There are 10 victims are injured in the volcanic eruption. However, the situation is handled well by the local authorities. So, there is no external aid requested.
5) Damage. For example: building collapse, loss of human lives.
 6) Change of social function: Cannot do daily life activities. For example: cannot go to school.
6) Change of social function: Cannot do daily life activities. For example: cannot go to school.
7) Disaster: A situation where external aids are needed in order to recover the whole situation back to normal. For example: Reconstruction of all this needs a large number of resources, funds included, which cannot be accomplished by local people and government. They need help.
How do we manage a disaster?

1) Prevention: It is defined by Dr. Hendro Wartatmo as a step to eradicate the hazard. Hence, prevention can only be done for man-made disaster, but not natural disaster.
2) Mitigation: It is an effort to reduce the risk as well as the impact of an event and the vulnerability of objects or individuals. For example: build earthquake-proof houses.
3) Preparedness: It is a step to increase the capacity of objects/ individuals in order to be able to manage the the impact of an event and lessen the damage after an event happens. So, it embraces measures which enable governments, communities and individuals to respond rapidly to disaster situations to cope with them effectively. It includes:
a) Formulate emergency plans. For example, establish hospital incident command system. It provides hospital with tools needed to advance their emergency preparedness and response capability. It allows personnel from different agencies or departments to be integrated into a common structure that can effectively address issues and delegate responsibilities. Besides that, it provides needed logistical and administrative support to operational personnel.
 Further reading of HICS: http://www.scha.org/images/stories/quality/hics_monograph.pdf
Further reading of HICS: http://www.scha.org/images/stories/quality/hics_monograph.pdf
b) Development of warning systems
c) The maintenance of inventories
d) The training of personnel. For example: train medical students for basic life support; train the personnel for psychological first aids: active listening, empathy, access the basic needs, don't force the victims to speak, avoid secondary stressors; train them to be able to identify people with depression, post-traumatic stress disorder or other psychological disorders.
4) Resilience: It consists of absorbing capacity, buffering capacity and response.
a) Absorbing capacity: According to Dr. Sulanto Saleh-danu R.,it can done to reduce the damage or prevent the event from causing damage. For example: build a dam to absorb the lava.
b) Buffering capacity: It is about how we cope with the impact and damage of the event. For example: We need logistic support in this step in order to support the organization and implementation of response, so that we can ensure the timeliness and efficiency. The logistic support can be: medicines, health supplies/kits, water and environmental health, food, logistic administration, shelter, electrical constructions, personal needs and education, human resources, agriculture, transportation and others.


How do we calculate the available resources?



Disaster is defined as sudden ecological phenomenon of sufficient magnitude to require external aids. It is also defined as an event or a series of events that are caused by natural factor or man-made factor, resulting in loss of human lives, environmental damage, loss of properties, and psychological problem. Consequently, human lives are harmed and disturbed.
Let's look at the conceptual framework of a disaster:

1) Hazard: Hazard is the cause of an event or a disaster. For example: the hazard of flood is the rain; the hazard of volcanic eruption is the volcano.
2) Risk: A factor which increases the probability of a hazard to become an event. For example: Deforestation will increase the probability of a flood to take place;
3) Event: It is caused by the hazard. For example: flood, volcano eruption.
4) Impact: When the event involves a population, but not yet a disaster. For example: There are 10 victims are injured in the volcanic eruption. However, the situation is handled well by the local authorities. So, there is no external aid requested.
5) Damage. For example: building collapse, loss of human lives.

7) Disaster: A situation where external aids are needed in order to recover the whole situation back to normal. For example: Reconstruction of all this needs a large number of resources, funds included, which cannot be accomplished by local people and government. They need help.
How do we manage a disaster?

1) Prevention: It is defined by Dr. Hendro Wartatmo as a step to eradicate the hazard. Hence, prevention can only be done for man-made disaster, but not natural disaster.
2) Mitigation: It is an effort to reduce the risk as well as the impact of an event and the vulnerability of objects or individuals. For example: build earthquake-proof houses.
3) Preparedness: It is a step to increase the capacity of objects/ individuals in order to be able to manage the the impact of an event and lessen the damage after an event happens. So, it embraces measures which enable governments, communities and individuals to respond rapidly to disaster situations to cope with them effectively. It includes:
a) Formulate emergency plans. For example, establish hospital incident command system. It provides hospital with tools needed to advance their emergency preparedness and response capability. It allows personnel from different agencies or departments to be integrated into a common structure that can effectively address issues and delegate responsibilities. Besides that, it provides needed logistical and administrative support to operational personnel.

b) Development of warning systems
c) The maintenance of inventories
d) The training of personnel. For example: train medical students for basic life support; train the personnel for psychological first aids: active listening, empathy, access the basic needs, don't force the victims to speak, avoid secondary stressors; train them to be able to identify people with depression, post-traumatic stress disorder or other psychological disorders.
4) Resilience: It consists of absorbing capacity, buffering capacity and response.
a) Absorbing capacity: According to Dr. Sulanto Saleh-danu R.,it can done to reduce the damage or prevent the event from causing damage. For example: build a dam to absorb the lava.
b) Buffering capacity: It is about how we cope with the impact and damage of the event. For example: We need logistic support in this step in order to support the organization and implementation of response, so that we can ensure the timeliness and efficiency. The logistic support can be: medicines, health supplies/kits, water and environmental health, food, logistic administration, shelter, electrical constructions, personal needs and education, human resources, agriculture, transportation and others.


How do we calculate the available resources?

c) Response. It is the activities done immediately after the event happens in order to handle and manage the negative impacts and damage. The activities includes:
- Rescue and evacuation of casualties. The medical response can be divided into prehospital and hospital. For prehospital stage, they need to do triage, resuscitation, stabilization. No definitive treatment is given. For hospital stage, they need to do the triage again (because the patient's condition may alter during the journey to hospital), resuscitation, stabilization and give definitive treatment.
- Fulfilment of basic needs.
- Protection, e.g. place the victims in a safe place.
- Management of refugee and dead bodies.
- Recovery of infrastructure and facilities.

5) Recovery, rehabilitation, reconstruction.
a) Recovery: It is the process, policies and procedures for recovery or continuation of technology and infrastructure critical to an organization after a disaster.
b) Rehabilitation: It is about the restoring and recovery of the public services and social functions, so that everything (the community's living and the administrative aspect) can be returned to the norm.
c) Reconstruction: Reconstruct the infrastructure, and institutions in order to restore and develop the economy, social and culture as well as the law and regulation in the region after the disaster.

In conclusion,
we as a doctor, can take part in preparedness, resilience and recovery. If a disaster happens and it is the 1st time in the country, there might be a lot of mistakes done and we might face a lot of shortages: e.g. hosp inable to provide enough medical supports or space to treat the victims, infections spread among the victims, etc. The important thing is WE HAVE TO LEARN FROM MISTAKEs, so that we will know what to do in the next time. That's how we will know what to do for the prevention, mitigation and preparedness.
we as a doctor, can take part in preparedness, resilience and recovery. If a disaster happens and it is the 1st time in the country, there might be a lot of mistakes done and we might face a lot of shortages: e.g. hosp inable to provide enough medical supports or space to treat the victims, infections spread among the victims, etc. The important thing is WE HAVE TO LEARN FROM MISTAKEs, so that we will know what to do in the next time. That's how we will know what to do for the prevention, mitigation and preparedness.
Reference:
1) Dr. Hendro Wartatmo. Lecture: Conceptual Framework of Disaster and Disaster Management.
2) Dr. Bambang Hastha Yoga. Lecture: Disaster Management in Mental Health.
3) Dr. Belladonna. Lecture: Preparedness, Response and Recovery.
4) Dr. Sulanto Saleh-danu R.. Lecture: Logistic (medical) and Disaster.
Motivation
How do I motivate my assistants or employees to work? This kind of question may always be asked by a leader.
Before answering this question, let's think about this: When will one be motivated to work? and why?
-Monetary gain?
-Self-satisfaction?
-Challenging job?
-Freedom?
-Treated fairly in workplace where there is no bias?
There are few theories explaining what motivation is. Let's read about the scenario below:
"Ann, I don't want to work at here any more.."
"Why? U have found a new job?"
"No, I just find it meaningless for working at this primary health care center. Everyone is doing their own work alone, without helping each other. And..you see, Mary and John are always late, while Carmen is always finding an excuse to go out to serve her private patients. Although they don't do their job well, they still get the same salary, as us. No matter how hard we work, there is no promotion and we don't get higher incentives. It is very unfair for us! I lose my motivation to work!"
Why does the girl want to quit the job? Because she is not treated fairly and the outcome she gets is not proportional to the effort she puts. So, in this scenario, it involves 2 theories: Equity theory and expectancy theory.
1) Equity theory.
It says that motivation will be enhanced if people think they are being treated fairly.
2) Expectancy theory.
It explains that motivation is a function of 3 distinct concepts:
a) Expectancy. It is based on the perceived effort-performance relationship. It is the expectancy that one's effort will lead to the desired performance and is based on past experience, self-confidence, and the perceived difficulty of the performance goal. For instance: If I work harder than others, will I produce more?
b) Instrumentality: It is based on the perceived performance-reward relationship. It is the belief that if one does meet performance expectations, he or she will receive a greater reward. For instance: If I produce more than anyone else, will I get a bigger raise or faster promotion?
c) Valence: It refers to value the individual personally places on the rewards. It can be one's needs, goals, values, money, etc. For instance: Do i want a bigger raise? is it worth the extra effort? Do I want a promotion?

In another words, motivation= expectancy x instrumentality x valence. In the scenario above, the worker does not perceive ''instrumentality". As a result, there is no motivation to work.
Are there any other theories? Read the following:
Dr. A is sent to puskesmas X to work. After several days, he finds that the medical record system is poor, and there is no one there to help him out, except 1 nurse. Some of the workers come to work late, but leave the puskesmas earlier than anyone else. When he asks the admin about the data, e.g. the top ten disease in that puskesmas, the time sheet of the workers, the admin can't show him any data about that. There is no teamwork, no management, and no health information. They don't communicate well with each other.
"Doctor, the working condition and the health system in this puskesmas are very poor. Why are you still enthusiastic about doing your job here?"
"Well, Ann, don't you think this is challenging? I am so glad that I finally get a very challenging task. I want to solve the problems here and then improve the health system of this puskesmas, including the management, within 6 months. I believe that I am able to do this".
After reading this scenario, can you answer why Doctor A is motivated to work? Because the job is challenging and he thinks that he is able to do so.
2 theories can be applied in this scenario: Goal theory and self-efficacy theory.
1) Goal theory.
It explains that motivation and performance are higher under 3 conditions: i) specific goals of individual; ii) goals are challenging and difficult to achieve; iii) feedback on performance.
2) Self-efficacy theory.
It explains that people are more likely to be motivated to do a better job if they believe they are able to do so.

In conclusion,
one can be motivated by intrinsic factors (e.g the goals, expectations, self-satisfaction, etc) and extrinsic factors (e.g money, promotion, benefits, etc). With the motivation, they can perform better when they are on duty. However, if one is not capable, and is not given a chance to work, no matter how one is motivated, they still cannot perform in the workplace.
So, train your workers, give them a chance to work, and motivate them! ;)
p/s: there are few more theories mentioned in the lecture note "motivation". So, remember to read it =)
Reference:
1) Dr. Andreasta Meliala. Lecture: Motivation.
2) http://www.12manage.com/methods_vroom_expectancy_theory.html
3)http://www.quickmba.com/mgmt/expectancy-theory/
Before answering this question, let's think about this: When will one be motivated to work? and why?
-Monetary gain?
-Self-satisfaction?
-Challenging job?
-Freedom?
-Treated fairly in workplace where there is no bias?
There are few theories explaining what motivation is. Let's read about the scenario below:
"Ann, I don't want to work at here any more.."
"Why? U have found a new job?"
"No, I just find it meaningless for working at this primary health care center. Everyone is doing their own work alone, without helping each other. And..you see, Mary and John are always late, while Carmen is always finding an excuse to go out to serve her private patients. Although they don't do their job well, they still get the same salary, as us. No matter how hard we work, there is no promotion and we don't get higher incentives. It is very unfair for us! I lose my motivation to work!"

Why does the girl want to quit the job? Because she is not treated fairly and the outcome she gets is not proportional to the effort she puts. So, in this scenario, it involves 2 theories: Equity theory and expectancy theory.
1) Equity theory.
It says that motivation will be enhanced if people think they are being treated fairly.
2) Expectancy theory.
It explains that motivation is a function of 3 distinct concepts:
a) Expectancy. It is based on the perceived effort-performance relationship. It is the expectancy that one's effort will lead to the desired performance and is based on past experience, self-confidence, and the perceived difficulty of the performance goal. For instance: If I work harder than others, will I produce more?
b) Instrumentality: It is based on the perceived performance-reward relationship. It is the belief that if one does meet performance expectations, he or she will receive a greater reward. For instance: If I produce more than anyone else, will I get a bigger raise or faster promotion?
c) Valence: It refers to value the individual personally places on the rewards. It can be one's needs, goals, values, money, etc. For instance: Do i want a bigger raise? is it worth the extra effort? Do I want a promotion?

In another words, motivation= expectancy x instrumentality x valence. In the scenario above, the worker does not perceive ''instrumentality". As a result, there is no motivation to work.
Are there any other theories? Read the following:
Dr. A is sent to puskesmas X to work. After several days, he finds that the medical record system is poor, and there is no one there to help him out, except 1 nurse. Some of the workers come to work late, but leave the puskesmas earlier than anyone else. When he asks the admin about the data, e.g. the top ten disease in that puskesmas, the time sheet of the workers, the admin can't show him any data about that. There is no teamwork, no management, and no health information. They don't communicate well with each other.
"Doctor, the working condition and the health system in this puskesmas are very poor. Why are you still enthusiastic about doing your job here?"
"Well, Ann, don't you think this is challenging? I am so glad that I finally get a very challenging task. I want to solve the problems here and then improve the health system of this puskesmas, including the management, within 6 months. I believe that I am able to do this".
After reading this scenario, can you answer why Doctor A is motivated to work? Because the job is challenging and he thinks that he is able to do so.
2 theories can be applied in this scenario: Goal theory and self-efficacy theory.
1) Goal theory.
It explains that motivation and performance are higher under 3 conditions: i) specific goals of individual; ii) goals are challenging and difficult to achieve; iii) feedback on performance.
2) Self-efficacy theory.
It explains that people are more likely to be motivated to do a better job if they believe they are able to do so.

In conclusion,
one can be motivated by intrinsic factors (e.g the goals, expectations, self-satisfaction, etc) and extrinsic factors (e.g money, promotion, benefits, etc). With the motivation, they can perform better when they are on duty. However, if one is not capable, and is not given a chance to work, no matter how one is motivated, they still cannot perform in the workplace.
So, train your workers, give them a chance to work, and motivate them! ;)
p/s: there are few more theories mentioned in the lecture note "motivation". So, remember to read it =)
Reference:
1) Dr. Andreasta Meliala. Lecture: Motivation.
2) http://www.12manage.com/methods_vroom_expectancy_theory.html
3)http://www.quickmba.com/mgmt/expectancy-theory/
Subscribe to:
Comments (Atom)